This is a virtual event. Please click here to register and generate a link to the talk.
The link will be unique to you; please save it and do not share with others.
To celebrate its May release, contributors Karen Eggleston, Barry Naughton, and Andrew Walder will join editors Thomas Fingar and Jean Oi for a panel discussion of their volume Fateful Decisions: Choices That Will Shape China’s Future (Stanford University Press). China has enjoyed an extraordinary run of rapid growth and development over the last 40 years. Yet, as Fingar and Oi point out, China’s future is hardly set in stone. Sustained economic growth, social welfare and stability will depend upon tough policy decisions confronting Beijing’s leaders today in what is a watershed moment. Casting doubt on Beijing’s aversion to major reforms and its return to certain Mao-era policy tools, Oi and Fingar argue that China’s challenges are not only complex, but high-stakes – challenges that have become even more daunting in the aftermath of COVID-19. As China battles the difficulties caused by an aging population, the loss of comparative economic advantage, a politically entrenched elite, and a population with rising expectations, today’s policy decisions will weigh heavily on its future. Topics explored in the volume include China's healthcare challenges in a slowing economy, its global ambitions and track record, economic aims and realities, the country’s mounting governance pressures, and more.
Fateful Decisions is available for purchase here.
Fore more information on Fateful Decisions, check out these articles:
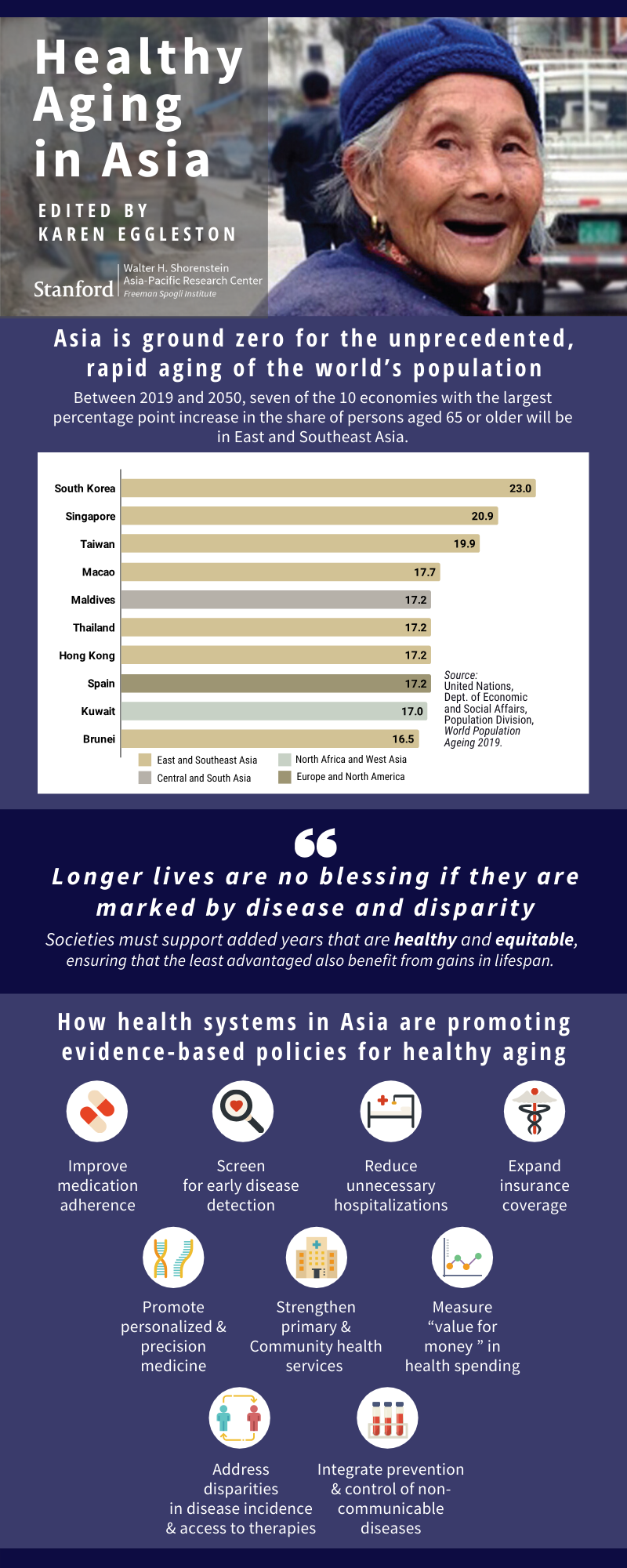
Karen Eggleston Examines China’s Looming Demographic Crisis, in Fateful Decisions
Now It Gets Much Harder: Thomas Fingar and Jean Oi Discuss China’s Challenges in The Washington Quarterly
China’s Challenges: Now It Gets Much Harder
 Karen Eggleston is a senior fellow at the Freeman Spogli Institute for International Studies (FSI) at Stanford University, director of the Stanford Asia Health Policy Program, and deputy director of the Walter H. Shorenstein Asia-Pacific Research Center at FSI. She is also a fellow with the Stanford Center for Innovation in Global Health and a faculty research fellow of the National Bureau of Economic Research (NBER). Eggleston earned her PhD in public policy from Harvard University, studied in China for two years, and was a Fulbright scholar in South Korea. Her research focuses on comparative health systems and health reform in Asia, especially China; government and market roles in the health sector; supply-side incentives; healthcare productivity; and economic aspects of demographic change.
Karen Eggleston is a senior fellow at the Freeman Spogli Institute for International Studies (FSI) at Stanford University, director of the Stanford Asia Health Policy Program, and deputy director of the Walter H. Shorenstein Asia-Pacific Research Center at FSI. She is also a fellow with the Stanford Center for Innovation in Global Health and a faculty research fellow of the National Bureau of Economic Research (NBER). Eggleston earned her PhD in public policy from Harvard University, studied in China for two years, and was a Fulbright scholar in South Korea. Her research focuses on comparative health systems and health reform in Asia, especially China; government and market roles in the health sector; supply-side incentives; healthcare productivity; and economic aspects of demographic change.
 Thomas Fingar is a Shorenstein Distinguished Fellow in the Shorenstein Asia-Pacific Research Center at Stanford University. From May 2005 through December 2008, he served as the first deputy director of national intelligence for analysis and, concurrently, as chairman of the National Intelligence Council. Previous positions include assistant secretary of state for Intelligence and Research (2000-2001, 2004–2005), principal deputy assistant secretary (2001–2003), deputy assistant secretary for analysis (1994–2000), director of the Office of Analysis for East Asia and the Pacific, and chief of the China Division. Fingar is a graduate of Cornell University (AB in government and history) and Stanford University (MA and PhD, both in political science). His most recent books are Uneasy Partnerships: China’s Engagement with Japan, the Koreas, and Russia in the Era of Reform (editor) (Stanford University Press, 2017); The New Great Game: China’s Relations with South and Central Asia in the Era of Reform (editor) (Stanford University Press, 2016); and Reducing Uncertainty: Intelligence Analysis and National Security (Stanford University Press, 2011).
Thomas Fingar is a Shorenstein Distinguished Fellow in the Shorenstein Asia-Pacific Research Center at Stanford University. From May 2005 through December 2008, he served as the first deputy director of national intelligence for analysis and, concurrently, as chairman of the National Intelligence Council. Previous positions include assistant secretary of state for Intelligence and Research (2000-2001, 2004–2005), principal deputy assistant secretary (2001–2003), deputy assistant secretary for analysis (1994–2000), director of the Office of Analysis for East Asia and the Pacific, and chief of the China Division. Fingar is a graduate of Cornell University (AB in government and history) and Stanford University (MA and PhD, both in political science). His most recent books are Uneasy Partnerships: China’s Engagement with Japan, the Koreas, and Russia in the Era of Reform (editor) (Stanford University Press, 2017); The New Great Game: China’s Relations with South and Central Asia in the Era of Reform (editor) (Stanford University Press, 2016); and Reducing Uncertainty: Intelligence Analysis and National Security (Stanford University Press, 2011).
Barry Naughton is the So Kwanlok Professor at the School of Global Policy and Strategy, University of California–San Diego. Naughton’s work on the Chinese economy focuses on market transition; industry and technology; foreign trade; and political economy. His first book,
Growing Out of the Plan, won the Ohira Prize in 1996, and a new edition of his popular survey and textbook,
The Chinese Economy: Adaptation and Growth, appeared in 2018. Naughton did his dissertation research in China in 1982 and received his PhD in economics from Yale University.
 Jean C. Oi is the William Haas Professor of Chinese Politics in the Department of Political Science and a senior fellow in the Freeman Spogli Institute for International Studies at Stanford University. She directs the China Program at the Walter H. Shorenstein Asia-Pacific Research Center and is the Lee Shau Kee Director of the Stanford Center at Peking University. Oi has published extensively on China’s reforms. Recent books include Zouping Revisited: Adaptive Governance in a Chinese County, coedited with Steven Goldstein (Stanford University Press, 2018), and Challenges in the Process of China’s Urbanization, coedited with Karen Eggleston and Yiming Wang (2017). Current research is on fiscal reform and local government debt, continuing SOE reforms, and the Belt and Road Initiative.
Jean C. Oi is the William Haas Professor of Chinese Politics in the Department of Political Science and a senior fellow in the Freeman Spogli Institute for International Studies at Stanford University. She directs the China Program at the Walter H. Shorenstein Asia-Pacific Research Center and is the Lee Shau Kee Director of the Stanford Center at Peking University. Oi has published extensively on China’s reforms. Recent books include Zouping Revisited: Adaptive Governance in a Chinese County, coedited with Steven Goldstein (Stanford University Press, 2018), and Challenges in the Process of China’s Urbanization, coedited with Karen Eggleston and Yiming Wang (2017). Current research is on fiscal reform and local government debt, continuing SOE reforms, and the Belt and Road Initiative.
 Andrew G. Walder is the Denise O’Leary and Kent Thiry Professor of Sociology in the School of Humanities and Sciences, and a senior fellow in the Freeman Spogli Institute for International Studies at Stanford University. A political sociologist, Walder has long specialized in the study of contemporary Chinese society and political economy. After receiving his PhD at the University of Michigan, he taught at Columbia, Harvard, and the Hong Kong University of Science and Technology. At Stanford he has served as chair of the Department of Sociology, director of the Asia-Pacific Research Center, and director of the Division of International, Comparative, and Area Studies in the School of Humanities and Sciences. His most recent books are Fractured Rebellion: The Beijing Red Guard Movement (2009), China under Mao: A Revolution Derailed (2015), and Agents of Disorder: Inside China’s Cultural Revolution (2019).
Andrew G. Walder is the Denise O’Leary and Kent Thiry Professor of Sociology in the School of Humanities and Sciences, and a senior fellow in the Freeman Spogli Institute for International Studies at Stanford University. A political sociologist, Walder has long specialized in the study of contemporary Chinese society and political economy. After receiving his PhD at the University of Michigan, he taught at Columbia, Harvard, and the Hong Kong University of Science and Technology. At Stanford he has served as chair of the Department of Sociology, director of the Asia-Pacific Research Center, and director of the Division of International, Comparative, and Area Studies in the School of Humanities and Sciences. His most recent books are Fractured Rebellion: The Beijing Red Guard Movement (2009), China under Mao: A Revolution Derailed (2015), and Agents of Disorder: Inside China’s Cultural Revolution (2019).










 Dr. Gendengarjaa Baigalimaa
Dr. Gendengarjaa Baigalimaa